Stretching and tissue expansion for face lift: five year experience
© 1992 Elsevier Science Publishers B.V. All rights reserved.
Plastic Surgery 1992. Vol. I. U.T. Hinderer, editor
Daniel Man
Boca Raton, Florida, U.S.A.
Purpose
The purpose of intraoperative stretching and expansion in facelift is to obtain circumferential relaxation and a natural look in contrast with a sometimes pulled look associated with standard face lifts. While removing more wrinkled skin, closure of the incisions is accomplished with decreased tension.
Methods and Techniques
Based on well established studies [1-5] I have further developed this technique [6]. Wide undermining is established beyond the deep nasolabial folds and the marionette lines in a superficial plane. Correction of the underlying fat, SMAS and platysma is obtained prior to stretching and expansion. The crescent shaped tissue expander* called the Man face lift expander is placed under the flaps next to the nasolabial folds and the marionette lines (Fig. 1). An estimate is made of the amount of skin available for resection compared with the fixed point of the earlobe. The stretch is achieved by having the anchor staples placed superior and posterior to the ear, under tension, into the hair-bearing area of the scalp. The tissue expander is inflated with air until the entire elevated flap is put under tension. The corners of the mouth are pushed mechanically with the finger medially underneath the flap rather than let them get pulled laterally.
The inflation is stopped and maintained at the same pressure for approximately one minute during the first load cycle to initiate the tissue creep. The expander is then deflated to permit tissue perfusion for approximately one to two minutes allowing for stress relaxation. This procedure is repeated two more times to a total of three times to allow additional air to be introduced, resulting in further expansion. The rapid intraoperative expansion for a very short duration allows circumferential relaxation of all the undermined flaps leading to push of the corners of the mouth medially and decreased tension on the anchor sutures laterally thereby achieving a more natural look. This technique allows better redraping of the skin of the face and neck. During inflation of the expander, the tubing is protruding through the preauricular face lift incision. The location ofdiscomfort. Normal sensation of the flaps was regained similar to the usual rhytidectomy after two to four months. There were no telangiectasias and no significant changes in hairline. Pigment changes were temporary in three patients.
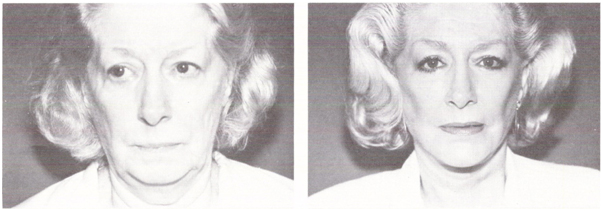
Fig. 1. Before secondary face lift.
Fig. 2. After secondary face lift.
Cox-Uphoff Company, Santa Barbara, California
Discussion
The new technique of using the Man face lift expander during rhytidectomy surgery provides significantly greater skin removal than the current approaches. I developed this technique in response to three problems that I observed occurring to one side of the face lift while proceeding with the other: (1) contracture and contraction that needs to be overcome later; (2) oozing beneath the elevated flap; and (3) wasted time in having to restretch what could have been stretched in the first place. In my opinion, intraoperative stretching and tissue expansion can be routinely used as an effective means to overcome contraction of the elevated soft-tissue flap that occurs with the standard face lift. By expanding one side of the face prior to proceeding to the other side, I was able to overcome the contracture and contraction that occurs while the flap that has been elevated is left alone as in the standard face lift. This immediate expansion also decreases oozing and bleeding associated with the usual rhytidectomy flap elevation by compressing the small capillaries in a tamponade fashion. Overall, the decrease in tension of the remaining flap thereby improves its viability, especially in the preauricular site, giving the patient a more natural appearance. I have observed, as Gibson had shown, that if the skin is repeatedly loaded, maximum expansion is not obtained at the first loading, since during the first load the amount of stretch is dependent on the initial displacement of fluid and ground substance in the dermis. After the repeated expansion, the skin stretches as the collagen and elastin fibers align themselves to the stress. After the stress is removed, the tissue returns to the slightly reduced size. The total result is additional gain of the skin-flap surface that lies in a more natural and circumferential manner when sutured to its final position. This is in contrast to an occasional stigma of a ‘pulled’ look of the usual rhytidectomy that is created by tension on the anchor sutures. The inflated expander at the level of the nasolabial fold allowed the corners of the mouth to be pushed medially toward each other. I call this phenomenon Circumferential Relaxation (Fig. 1) for its final appearance. Additional studies are warranted with regard to the timing and degree of expansion in facelifts. I would caution the user of this technique in the old, aged, thin and scarred skin. In these types of cases, I suggest careful decrease of the duration of skin pallor during stretching and expansion. I have no doubt that there are inherent dangers of abuse in any technique. This technique, that I have developed, although it appears to be simple and safe, is no exception.
Conclusion
Intraoperative stretching and expansion of rhytidectomy flaps has been performed successfully in 134 patients with only minor complications, as mentioned earlier. This technique can be implemented quickly and with ease during standard rhytidectomy. This technique is especially useful in patients who are prone to problems with tension on the flaps, such as in smokers or in secondary rhytidectomies (Fig. 2), and in sun damaged skin with many wrinkles. This procedure results in the additional removal of skin from the face in a safe, simple and uncomplicated manner. Though the technique has been used for only five years it is my impression, and my hope that the long term results may defer the need for additional face lifts for a longer period than the conventional rhytidectomy.
References
- Gibson T (1977) The Physical Properties of skin. In: Converse JM (ed.), Reconstructive Plastic Surgery, Vol. 1. Saunders, Philadelphia, pp. 70-77.
- Hirshowitz B and Jackson IT (1987) An attempt to harness the viscoelastic properties of skin in face lift operations: A preliminary report. Ann. Plast. Surg. 18: 188.